

The part of the brain most commonly targeted in TMS therapy for depression is the left dorsolateral prefrontal cortex (DLPFC), a region closely tied to mood, motivation, and emotional regulation.
When this part of the brain is underactive, which is common in depression, it can cause low energy, hopelessness, and mental fog. These symptoms make daily life harder to manage. TMS sends gentle magnetic pulses to stimulate that underactive area. This helps the brain reset how it handles mood. But the exact spot matters. Even a small shift can affect how well the treatment works. That’s why precision is key to making TMS effective.
TMS for Depression Targets the Left Dorsolateral Prefrontal Cortex (DLPFC)
TMS for depression targets the left dorsolateral prefrontal cortex (left DLPFC) more than any other brain area.
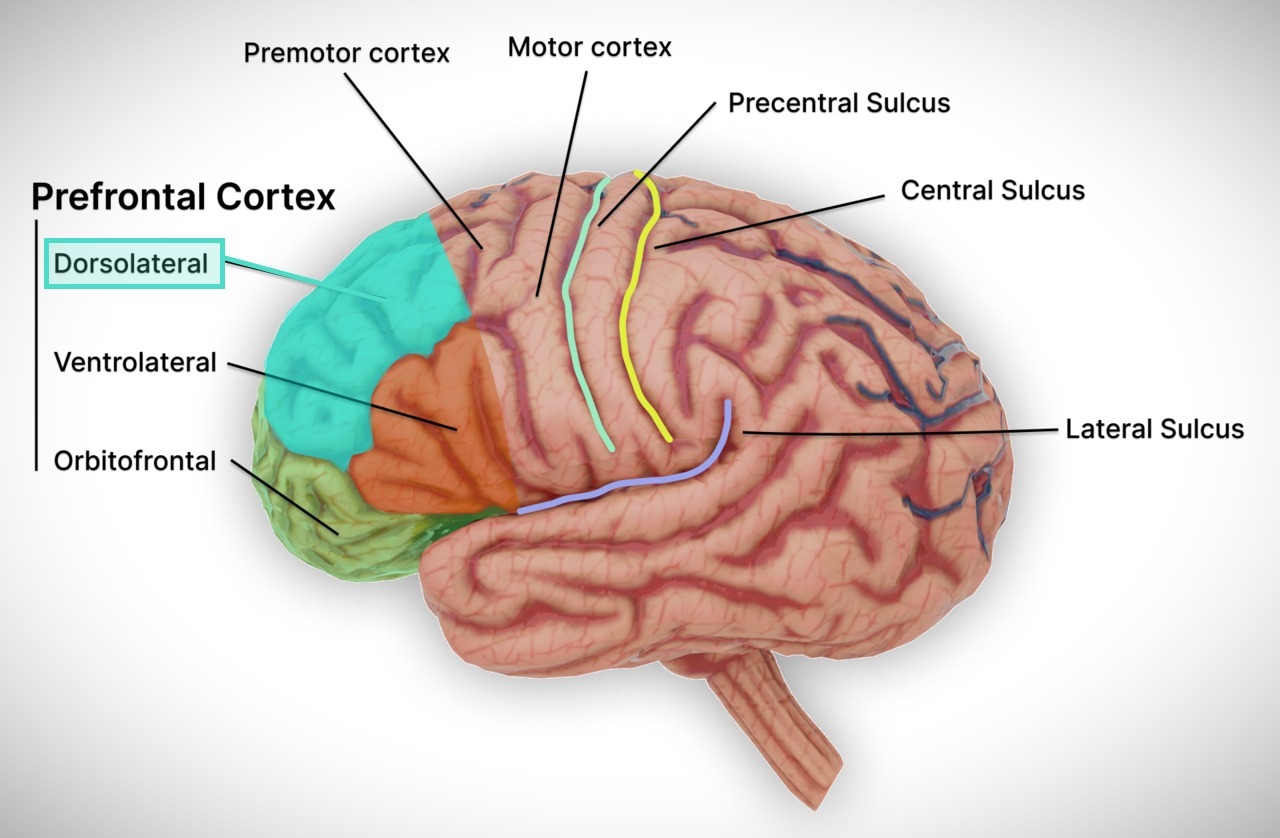
The prefrontal cortex sits just behind your forehead. It’s responsible for planning, focus, decision-making, and impulse control. The dorsolateral portion, specifically the left dorsolateral prefrontal cortex (left DLPFC), is deeply involved in regulating mood and emotional responses.
In people with depression, the left DLPFC often shows reduced activity. Brain scans frequently reveal it’s underactive, producing fewer electrical signals than it should. This underactivation can lead to:
- Poor concentration
- Low motivation
- Negative self-perception
- Emotional numbness
TMS aims directly at the left DLPFC to get it working again. The magnetic pulses help the brain cells in that area fire more often and more smoothly. With repeated sessions, this helps wake up the brain’s mood system and get things back in balance.
Over multiple sessions, this change can “retrain” the brain.
Why Is the Left DLPFC Chosen Over Other Areas?
The left DLPFC is chosen because it acts as a regulatory hub between emotional and cognitive systems.
When healthy, it helps suppress negative emotions and promotes positive, goal-directed behavior.
And as mentioned, when underactive, the brain’s emotional centers, especially the amygdala, become overactive, resulting in overwhelming sadness, fear, or helplessness.
Several reasons explain why the left DLPFC is preferred:
- Direct linkage to mood control: It connects to subcortical structures responsible for emotional responses.
- Easier access: Being on the brain’s surface makes it accessible to magnetic fields without invasive procedures.
- Proven clinical outcomes: Decades of clinical trials have shown that stimulating this area leads to measurable improvements in depressive symptoms.
Importantly, stimulating the left DLPFC helps lift mood by boosting positive emotions. In certain cases, the right DLPFC is targeted instead to help reduce anxiety. This emphasizes how each side of the brain influences emotional states in its own way.
What Other Brain Areas Are Involved?
While the left DLPFC is the primary target, it doesn’t work alone. Stimulating the DLPFC sets off a chain reaction across other key brain regions:
- Subgenual anterior cingulate cortex (sgACC) – Often hyperactive in depression; calming it may be key to recovery
- Amygdala – Processes fear and emotion; better DLPFC function helps regulate it
- Striatum – Related to reward and motivation; may contribute to improvements in anhedonia
- Default mode network (DMN) – Involved in rumination and self-focus. TMS appears to reduce overactivity here.
So, while the DLPFC is the “entry point,” the benefits ripple outward across a broader depression-related brain network.
Can TMS Target Other Brain Regions for Different Symptoms?
Using TMS to target other brain areas, depending on the condition being treated.
- Right DLPFC: Often stimulated in anxiety disorders to help reduce hyperactivity linked to worry and rumination.
- Motor cortex: Targeted in chronic pain syndromes, such as fibromyalgia, to modulate pain perception pathways.
- Auditory cortex: Targeted for treatment of auditory hallucinations in schizophrenia, aiming to reduce the severity and frequency of hallucinations.
- Medial prefrontal cortex: Under study for obsessive-compulsive disorder (OCD) to modify rigid, intrusive thought patterns.
Deep TMS (dTMS) technology, using specialized H-coils, can reach broader and deeper brain regions, offering new options for treatment-resistant depression, breaking nicotine dependence, and even PTSD.
How Does Brain Imaging Improve TMS Targeting?
Modern TMS clinics no longer rely solely on the “5 cm rule” from the motor cortex. Instead, they often use MRI, functional MRI (fMRI), or EEG-based systems to pinpoint the exact spot that needs stimulation.
Benefits of imaging-guided TMS include:
- Individualized treatment: Every brain has a unique shape and size. Imaging ensures the target fits the patient, not a template.
- Improved accuracy: MRI allows precise localization of the DLPFC and its functional connections.
- Reduced variability: Imaging minimizes the risk of missing the ideal stimulation site by accounting for skull thickness and brain asymmetries.
- Predictive value: Pre-treatment imaging can predict which patients are more likely to respond based on brain connectivity patterns.
A large study comparing traditional cap-based placement to neuronavigation showed that cap-based targeting was, on average, over 10 mm off-target. Neuronavigation reduced this error to less than 1 mm and delivered more consistent stimulation intensity. The study concluded that neuronavigation greatly improves accuracy, consistency, and the amount of stimulation reaching the intended brain region (1).
In short, imaging makes TMS more personal and more effective.
What Happens If the Wrong Area Is Stimulated?
If the magnetic pulses stimulate the wrong area, even by a few millimeters, outcomes can be weaker, slower, or completely absent.
Potential consequences of inaccurate stimulation include:
- Minimal symptom improvement: Patients may not feel noticeable changes even after completing a full course.
- Delayed response: Benefits may take longer to appear, requiring additional sessions or adjustments.
- Higher relapse risk: Poorly stimulated circuits may fail to sustain remission over time.
- Increased frustration and financial burden: Patients might need retreatment or alternative therapies, adding costs and emotional stress.
Fortunately, modern TMS clinics use neuronavigation systems and brain imaging to minimize these risks.
How Many Sessions Are Needed to Activate the Brain Fully?
TMS requires multiple sessions to build up cumulative effects in the brain’s neural networks.
The standard protocol involves:
- 30 to 36 sessions delivered five days a week over six to seven weeks.
- Each session lasts around 20 to 40 minutes, depending on stimulation frequency.
Why so many sessions?
Neuroplasticity, the brain’s ability to change and form new connections, takes time.
Repeated magnetic stimulation strengthens synaptic pathways between neurons, gradually restoring healthier brain function.
Skipping sessions, shortening the treatment plan, or stopping early can significantly reduce the chances of full recovery.
Can Brain Targeting Evolve in the Future?
Absolutely. The field is moving toward:
- Individualized targeting using patient-specific brain imaging
- Functional connectivity maps to identify the most responsive areas
- Closed-loop TMS that adapts stimulation based on real-time brain activity
In short, TMS is becoming smarter, faster, and more precise. But the core concept remains the same: stimulate the brain region that controls mood—and do it with accuracy.
We Don’t Guess. We Target. Find Out How We Get Real Results
We know that where TMS is delivered matters. That’s why our team targets the part of the brain that’s often underactive in people with depression. Every treatment follows proven protocols based on clinical studies. No guessing. Just consistent, precise coil placement guided by training, not shortcuts.
What makes our program stand out is experience. Our medical team has helped hundreds of people who didn’t improve with medication finally get relief through TMS. The results speak for themselves. Clearer thinking, better mood, and life back on track. If you’re ready to see what precision TMS can do, reach out to the TMS Institute of Arizona. We’re here to help you feel like yourself again.
References
- Caulfield, K. A., Fleischmann, H. H., Cox, C. E., Wolf, J. P., George, M. S., & McTeague, L. M. (2022). Neuronavigation maximizes accuracy and precision in TMS positioning: Evidence from 11,230 distance, angle, and electric field modeling measurements. Brain Stimulation, 15(5), 1192–1205. https://doi.org/10.1016/j.brs.2022.08.013


















