

TBI vs. PTSD in Veterans: Are We Misdiagnosing Brain Injuries?
Traumatic brain injury (TBI) and post-traumatic stress disorder (PTSD) are both unfortunately common in military combat veterans. Both affect brain function, emotions, and physical health, making diagnosis tough. Sometimes, PTSD cases are actually undiagnosed TBIs. Misdiagnosis happens more than expected. Could thousands of veterans be receiving treatment for the wrong condition? And does it matter – how do treatment approaches differ for the two conditions?
What Are the Differences Between PTSD and TBI?
PTSD develops after extreme stress, combat, or life-threatening events. Brain function changes, making it harder to process emotions. Fear, memory, and decision-making centers are most affected.
TBI is a physical injury to the brain, often from a blast, head impact, or sudden jolt. It damages brain tissue, leading to problems with thinking, mood, and movement.
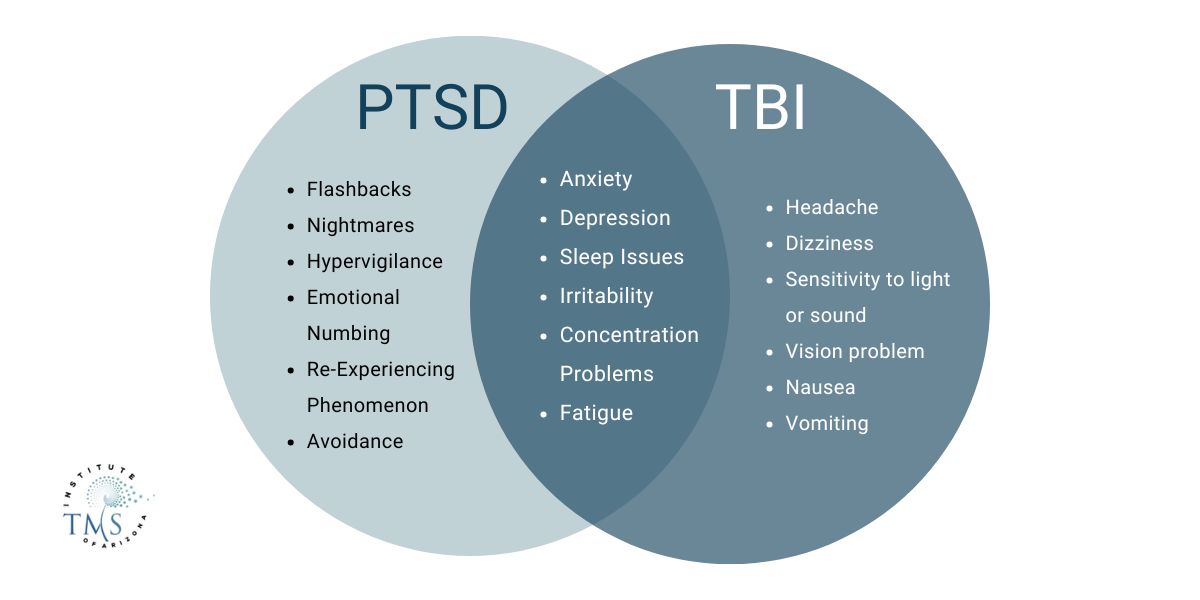
Key Differences:

Memory problems, concentration issues, irritability, and sleep disturbances overlap in both conditions. That makes diagnosis harder and often leads to confusion.
Why Are TBI and PTSD Often Confused?
Symptoms look alike, making it easy to mix up the two conditions. Standard tests often miss mild TBIs, and many veterans have both at the same time.
1. Overlapping Symptoms
Both TBI and PTSD can cause:
- Memory issues and concentration difficulties
- Mood swings, anxiety, and depression
- Insomnia and nightmares
- Irritability and impulsivity
Similar symptoms often lead to PTSD being diagnosed instead of TBI. Missing a head injury in medical records makes misdiagnosis even more likely.
2. Standard Medical Scans Miss Mild TBIs
- MRIs and CT scans may fail to detect microscopic brain damage from blast exposure.
- Newer imaging techniques like Diffusion Tensor Imaging (DTI) and functional MRI (fMRI) are emerging techniques that can detect subtle brain injuries but are not yet widely used in routine screenings.
A nearby explosion can cause a mild TBI, even if the service member was protected by an armored vehicle and no visible injury appears. Normal scans may lead doctors to mistake it for PTSD.
3. Delayed Onset of Symptoms
- TBI symptoms may not appear immediately. Veterans who sustain head trauma often don’t realize they have a brain injury until weeks or months later.
- PTSD symptoms can also be delayed, emerging long after combat exposure.
Neurological testing is needed to tell the difference between brain injury and psychological trauma. Without it, emotional and cognitive struggles can be misdiagnosed.
4. Misconceptions About PTSD and TBI
- PTSD is more widely recognized, and veterans with emotional distress often receive automatic PTSD diagnoses without full neurological evaluations.
- TBI is still poorly understood, especially when there’s no visible injury.
Veterans may accept a PTSD diagnosis rather than push for more in-depth brain injury testing.
How Many Veterans Have TBI and PTSD?
Many U.S. veterans deal with both Traumatic Brain Injury (TBI) and Post-Traumatic Stress Disorder (PTSD), especially those exposed to combat. The Department of Veterans Affairs says about 7% of all veterans will have PTSD at some point (1).
For those who served in Iraq and Afghanistan, about 20% have PTSD (2). From 2000 to 2021, over 450,000 service members were diagnosed with at least one TBI (3). Mild TBIs are more likely to be linked to PTSD than more severe brain injuries. This shows how important it is to address both conditions together to improve veterans’ well-being.
Did “Shell Shock” Mask Early Cases of TBI?
Yes, many cases of Traumatic Brain Injury (TBI) in World War I soldiers were likely misdiagnosed as shell shock. The funny thing about the term “shell shock” being used to describe PTSD is that it refers to trauma caused by nearby explosions, which is in fact, likely to cause TBI more than PTSD. At the time, the medical field lacked the knowledge and technology to distinguish between psychological trauma (now known as PTSD) and physical brain injuries caused by explosions.
Why Were TBIs Misdiagnosed as Shell Shock?
- Explosive Blasts and Brain Damage
The term “shell shock” was first used in 1915 because doctors believed artillery blasts caused symptoms like confusion, tremors, and fatigue. However, many soldiers who reported these symptoms had no visible injuries, making it difficult to diagnose brain damage. - Overlapping Symptoms
Both PTSD and TBI cause memory loss, dizziness, headaches, anxiety, and trouble concentrating. Without brain scans, doctors could not determine whether symptoms came from psychological trauma or a physical brain injury. - Stigma and Military Pressure
Soldiers with shell shock were often labeled as weak or cowardly. The British Army banned the diagnosis in 1917 to keep soldiers in combat. Many were sent back to battle without proper treatment, worsening their conditions.
Modern Evidence of TBI
Scientific research now confirms what WWI soldiers once described as suffering from shell shock, a condition long believed to be purely psychological, was likely traumatic brain injury (TBI) from repeated blast exposure.
A 2015 study by Johns Hopkins University examined the brains of modern combat veterans exposed to improvised explosive devices (IEDs) (4). Researchers found a distinct injury pattern in regions responsible for decision-making, memory, and reasoning. These findings suggest that many WWI soldiers suffering from shell shock may have experienced undiagnosed TBIs, rather than solely psychological trauma.
Further evidence comes from a 2024 study by the Uniformed Services University of the Health Sciences, which analyzed the brains of deceased service members (5). The research revealed that those exposed to repeated blast waves exhibited astroglial scarring in critical areas of the brain, including the gray-white matter junctions, cortical blood vessels, and ventricular linings. Even in cases of acute blast exposure, early signs of brain scarring were present.
These findings confirm that repeated blast exposure can lead to lasting neurological damage, reinforcing the idea that many early cases of shell shock were actually TBIs that went unrecognized for decades.
The Consequences of Misdiagnosing TBI as PTSD
Failing to recognize TBI means veterans may receive the wrong treatment.
- PTSD Treatment: Therapy, SSRIs, and exposure-based treatments.
- TBI Treatment: Neurological rehab, cognitive therapy, and brain stimulation treatments like TMS and MeRT.
Without proper care, untreated TBIs can worsen over time, leading to chronic migraines, neurodegenerative diseases, and increased suicide risk.
Could PTSD and TBI Occur Together?
Yes, PTSD and TBI often happen together, especially in combat veterans. Research from the U.S. Department of Veterans Affairs (VA) shows that TBI increases the risk of PTSD. A study found that 31.6% of severely injured combat veterans had moderate or severe TBI (6). Many of them also developed PTSD.
TBI can worsen PTSD symptoms by damaging memory, emotional control, and stress regulation. PTSD can also slow TBI recovery, leading to more anxiety, sleep problems, and depression. Veterans with both conditions face a higher risk of long-term disability. Substance abuse and suicide rates are also higher in those with both diagnoses.
How Do PTSD and TBI Overlap?
PTSD and TBI affect different parts of the brain, but their symptoms often look the same.
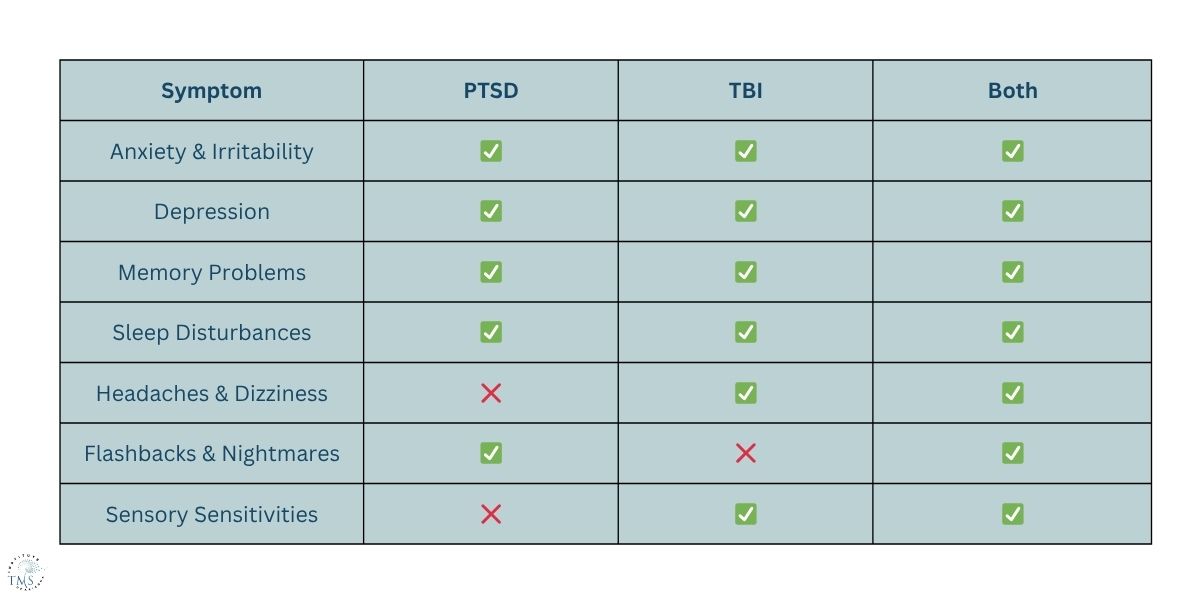
This symptom overlap leads to misdiagnosis. A veteran may receive PTSD treatment when their real issue is brain injury, or vice versa.
The Vicious Cycle of PTSD and TBI
- TBI can increase PTSD risk. Brain injuries affect the amygdala, which regulates fear. A damaged amygdala makes it harder to control anxiety, stress, and emotional regulation, worsening PTSD.
- PTSD can worsen TBI symptoms. Chronic stress from PTSD exacerbates cognitive issues in veterans with TBI. Sleep deprivation, anxiety, and depression make it harder to heal from brain injuries.
- Both conditions heighten suicide risk. Veterans with PTSD and TBI are more likely to experience severe depression and suicidal thoughts compared to those with just one condition.
What Happens When a Veteran Is Misdiagnosed?
The wrong treatment can lead to major health risks. Untreated TBI increases the chance of developing dementia and Alzheimer’s later in life. Misdiagnosed PTSD can push veterans toward substance abuse, depression, and worsening cognitive issues.
Many experience chronic pain, dizziness, and memory problems that affect their work and relationships. Additionally, a misdiagnosis also affects VA disability benefits. A veteran diagnosed with PTSD instead of TBI may get different disability ratings and less financial support.
Seeking Help for PTSD or TBI?
The TMS Institute of Arizona provides brain stimulation therapy for both PTSD and TBI. Many veterans struggle with symptoms that standard treatments haven’t improved.
Transcranial Magnetic Stimulation (TMS) supports mood regulation, cognitive function, and emotional stability. When PTSD treatment hasn’t worked or past brain injuries affect daily life, other treatments are available. Schedule a consultation with us.
References
- VA.gov | Veterans Affairs. (2024). Va.gov. https://www.ptsd.va.gov/understand/common/common_veterans.asp
- Vets, non-vets work together to understand PTSD. (2022, November 14). NSF – National Science Foundation. https://www.nsf.gov/science-matters/vets-non-vets-work-together-understand-ptsd
- CDC. (2025, January 31). Health Disparities in TBI. Traumatic Brain Injury & Concussion. https://www.cdc.gov/traumatic-brain-injury/health-equity/index.html
- Combat veterans’ brains reveal hidden damage from IED blasts. (2015). ScienceDaily. https://www.sciencedaily.com/releases/2015/01/150114140600.htm
- Shively, S. B., Horkayne-Szakaly, I., Jones, R. V., Kelly, J. P., Armstrong, R. C., & Perl, D. P. (2016). Characterisation of interface astroglial scarring in the human brain after blast exposure: a post-mortem case series. The Lancet Neurology, 15(9), 944–953. https://doi.org/10.1016/s1474-4422(16)30057-6
- Chin, D. L., & Zeber, J. E. (2019). Mental Health Outcomes Among Military Service Members After Severe Injury in Combat and TBI. Military Medicine, 185(5-6), e711–e718. https://doi.org/10.1093/milmed/usz440


















